

Benign prostatic Hyperplasia (BPH) is health problem that can occur with increasing the age in men, it is also called enlarged prostate. It is most common cause of urinary obstruction in men over 50 years of age.
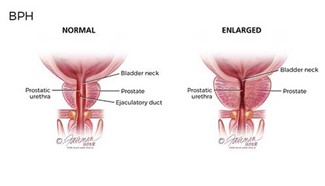
The sign of BPH is including frequency of urination, retention of urine, decrease in the diameter and pressure of urine flow and dribbling of the end of urine.
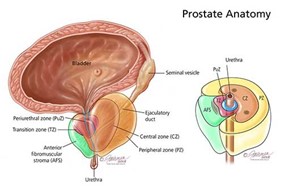
According to the medical history and PSA test and digital rectal examination (DRE) the urologist can diagnosis this disease. The evaluation this disease is summarized in figure 1.
The treatment of BPH according to the guidelines is different. For patients with mild symptoms, the recommended treatment is watchful waiting, then if the quality of life in patients does not improve, the doctors should consider pharmacotherapy.
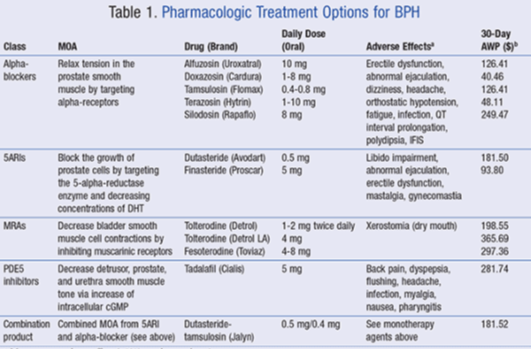
The current pharmacotherapy option for BPH management is alpha-adrenergic antagonists (alpha-blockers), 5-alpha-reductase inhibitors (5ARIs), muscarinic receptor antagonists (MRAs), and phosphodiesterase 5 (PDE5) inhibitors.
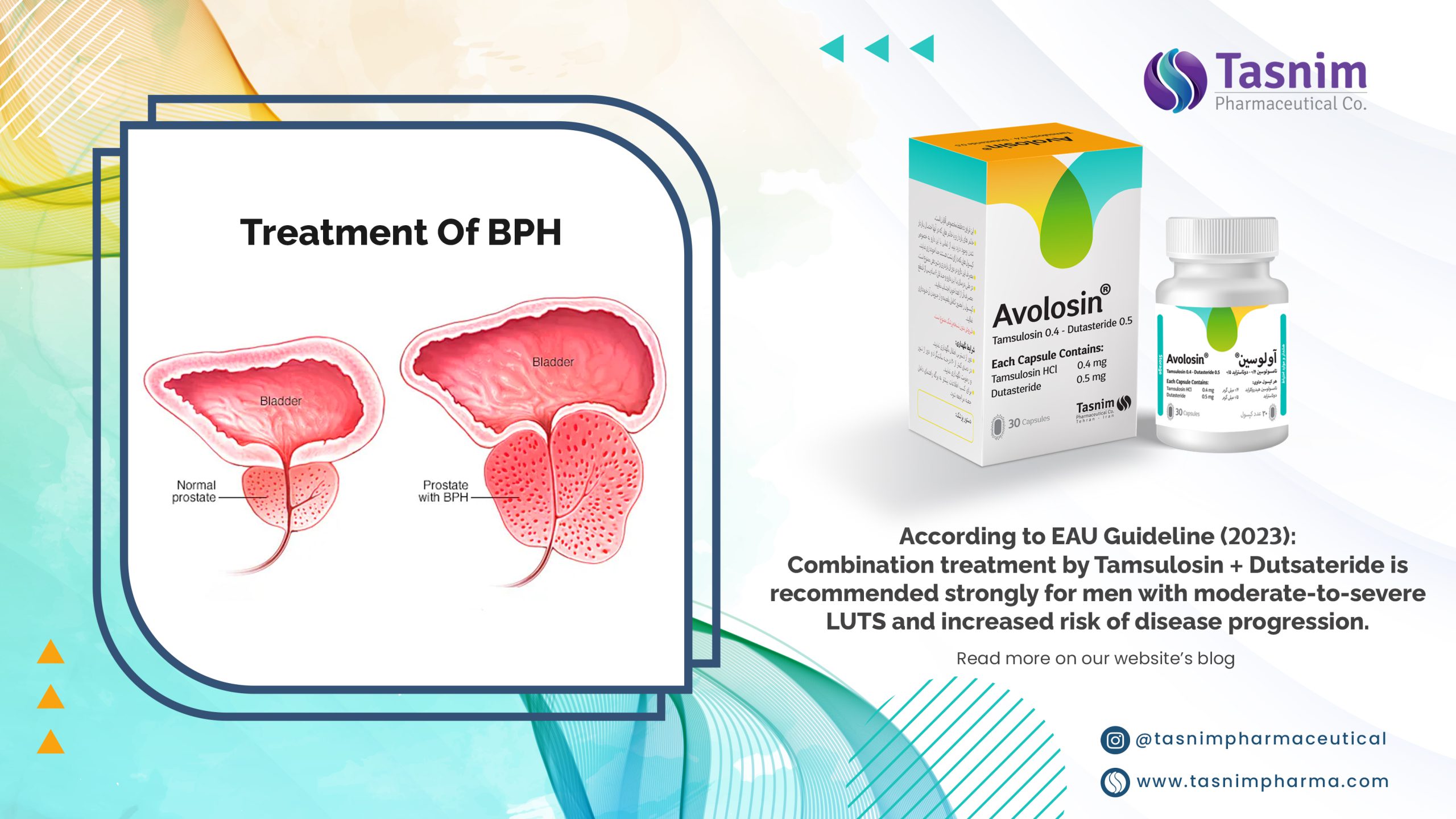
According to the clinical studies & new protocol in guidelines recommended the combination therapy in BPH patients. Combination therapy for LUTS/BPH includes 𝜶-adrenergic blockers and anticholinergic receptor blockers, 𝜶-adrenergic blockers and 𝜷𝟑-agonists, 𝜶-adrenergic blockers and phosphodiesterase type 5 inhibitors, 𝜶-adrenergic blockers and 5𝜶-reductase inhibitors.
Pursuant to the combAT and MTOPS study the combination therapy (𝜶-adrenergic blockers and 5𝜶-reductase inhibitors) is superior to monotherapy in clinical progression of BPH and the result is great improvement in LUTS.
According to the EAU 2023 Guideline:

References:
-
Roehrborn CG. Benign prostatic hyperplasia: an overview. Rev Urol. 2005;7(suppl 9):S3-S14.
-
McVary KT, Roehrborn CG, Avins AL, et al. American Urological Association Guideline: Management ofBenign Prostatic Hyperplasia (BPH). Linthicum, MD: American Urological Association; 2010:1-62, Appendix278-285.www.auanet.org/education/guidelines/benign-prostatic-hyperplasia.cfm. Accessed March 14, 2016.
-
3EAU Guidelines on Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO), J.N. Cornu (Chair), M. Gacci et al, UPDATE MARCH 2023, © European Association of Urology 2023.
-
Lepor H. Pathophysiology, epidemiology, and natural history of benign prostatic hyperplasia. Rev Urol.2004;6(suppl 9):S3-S10.
-
Abrams P, Chapple C, Khoury S, et al. Evaluation and treatment of lower urinary tract symptoms in oldermen. J Urol. 2009;181(4):1779-1787.

It is very efective with low complication.It is combinatin of two drug so the patients can take two drugs in a single pill andit is more convenient for them
no better than tamulosin
One pill versus two pills ! is a great choice for peoples who must eat multiple drugs during the day !